
*This webpage content is intended for Healthcare Professionals only, not for general public.
World Obesity Day is not just a day to raise awareness — it is a reminder to rethink how we define success in obesity care.
For too long, obesity has been reduced to a number on the weighing scale. Lose weight, and the treatment is considered effective. But obesity is now recognised globally as a chronic, relapsing disease, shaped by complex interactions between biology, metabolism, environment, and behaviour. Managing it requires more than rapid weight reduction — it demands long-term, health-focused strategies.
As new therapies reshape the treatment landscape, the distinction between weight loss and true improvements in body composition has never been more important.
GLP‑1 Therapies: A Turning Point in Obesity Treatment

The rise of GLP‑1 receptor agonists, including semaglutide and tirzepatide, marks a major turning point in obesity management. Originally developed for diabetes, these medications help regulate appetite, slow gastric emptying, and improve insulin sensitivity — mechanisms that directly address the biological drivers of obesity.
For many individuals, GLP-1 therapies enable substantial weight loss, with reductions of up to 15–20% of body weight within a year, alongside improvements in glycaemic control.
Yet as these treatments gain popularity, an important clinical question is emerging:
What exactly are patients losing — fat, muscle, or water?
When Weight Loss Comes at a Cost
While these GLP-1 therapies effectively reduce appetite and drive weight loss, clinical studies show that a substantial portion of weight lost may come from lean mass rather than fat, highlighting the need for careful monitoring:
- Wilding et al., NEJM 2021 (semaglutide): Average 15% weight loss, but nearly 40% of the lost weight came from lean mass.
- Rosenstock et al., NEJM 2021 (tirzepatide): Up to 20% weight loss, with significant muscle loss alongside fat loss.
- Lundgren et al., Lancet 2021: Individuals who stopped semaglutide regained weight, and much of the regain was fat rather than muscle.
Shifting the Focus: From Weight Reduction to Monitoring Body Composition
Modern obesity care is moving toward a more meaningful goal: monitoring body composition.
Rather than asking how much weight a patient has lost, clinicians are increasingly asking:
- Has fat mass been reduced?
- Has muscle mass been preserved?
- Is metabolic health improving?
This shift supports more personalised care and aligns treatment outcomes with real physiological improvements, not just cosmetic change.
InBody in Guiding Safe and Effective GLP-1 Weight Loss
Even with highly effective GLP-1 medications, achieving safe and sustainable weight loss requires losing fat while preserving muscle and metabolic health.
So, this is where InBody comes in to make a difference**. It provides clinicians with a detailed view of tissue-level changes, helping ensure that weight loss reflects real health improvements, not just numbers on the scale.
Here are the key InBody parameters to follow throughout treatment:
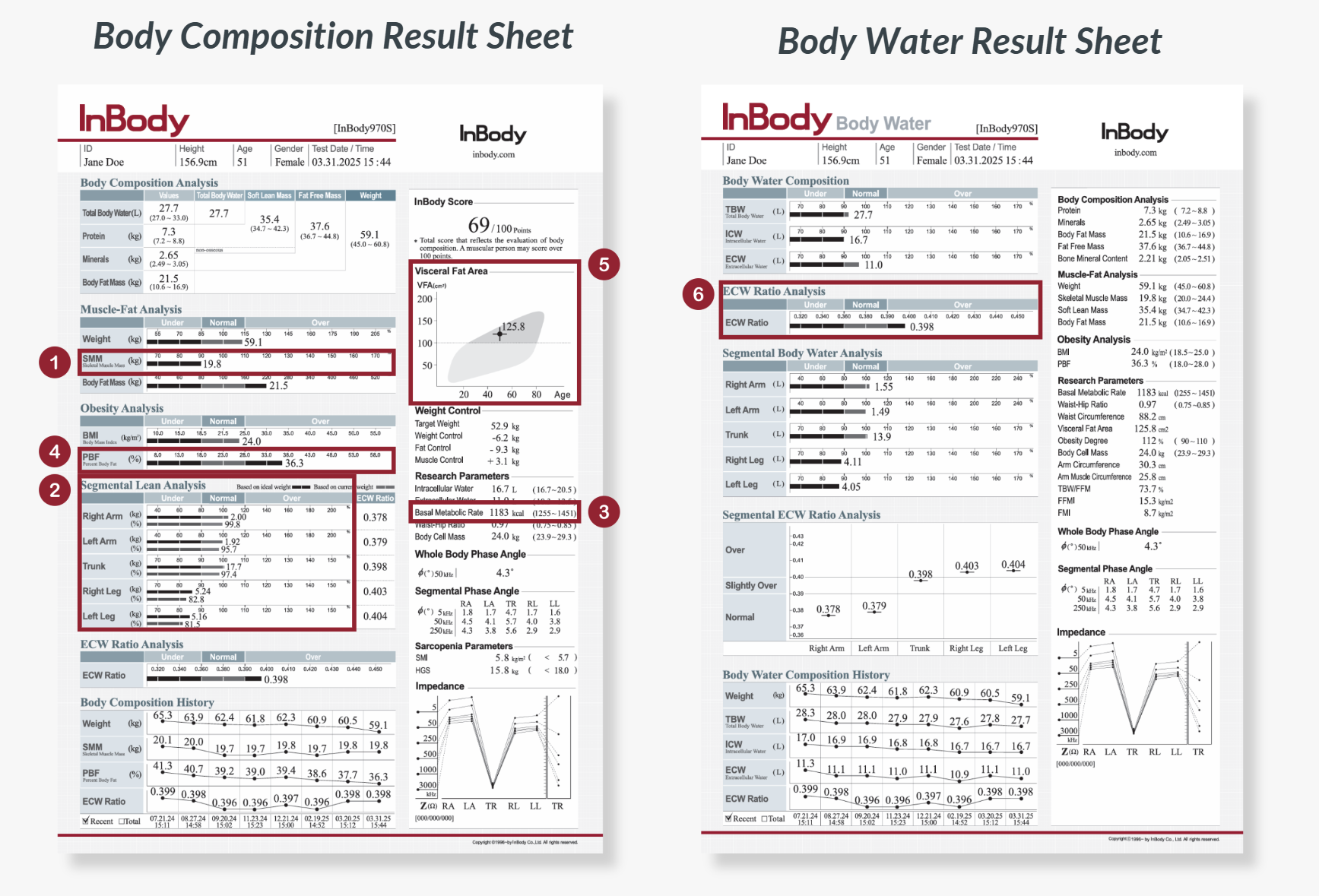
1. Skeletal Muscle Mass (SMM)
Measures total skeletal muscle mass responsible for strength, glucose uptake, and resting energy expenditure. Monitoring SMM ensures weight reduction comes from fat, not the muscle needed to maintain metabolic health and prevent frailty.
2. Segmental Lean Analysis
Shows muscle distribution across each limb and the trunk. It is useful in guiding targeted resistance exercises to preserve muscle where function matters most, especially in older adults vulnerable to sarcopenia.
3. Basal Metabolic Rate (BMR)
Indicates the number of calories needed by the body to sustain basic bodily functions. A declining BMR signals excessive loss of muscle mass, and a higher likelihood of weight regain once medication stops or dosage changes.
4. Percent Body Fat (PBF)
Represents fat relative to total body weight. PBF offers a clearer picture of true obesity improvement, especially when scale weight includes shifts in water.
5. Visceral Fat Area
Measures harmful fat around abdominal organs that drives inflammation, insulin resistance, and cardiovascular disease. GLP-1s specifically target visceral adiposity, making this a crucial marker of treatment success.
6. Extracellular Water (ECW) Ratio
InBody measures intracellular and extracellular water directly using multiple low and high frequencies. From this, the ECW Ratio is calculated to assess body water balance. An elevated ECW Ratio may indicate fluid retention or inflammation, which can make it harder to see real fat-loss progress because lean mass is overestimated.
Conclusion: A More Sustainable Path Forward
Effective obesity care does not end when the scale reaches a target number. Long-term success depends on maintaining muscle, preserving metabolic health, and supporting functional capacity.
On this World Obesity Day, the message is clear:
Weight loss alone is not the goal. Better health is.
By combining evidence-based therapies like GLP-1 medications with body composition monitoring, clinicians can deliver more precise, patient-centred, and sustainable obesity care!
Read our full blog on ‘Why Body Composition Matters More Than Ever in GLP-1 Weight loss?’






